Sai Santhoshini Achi, MD
Internal Medicine Resident at Harlem Hospital
Incoming Nephrology Fellow at University of Texas Health Science Center at Houston
@SaiAchi1
On the first day of my inpatient medicine rotation, I had three patients with dialysis catheters. I kept confusing the differences between tunneled and non-tunneled catheters and couldn’t remember which type of catheter they had. I wanted to explore more about the catheters and share those pearls of knowledge with other junior trainees.
Dialysis catheters are transcutaneous conduits used to gain access to the intravascular or intraperitoneal spaces as a means for kidney replacement therapy. Catheters can be classified into extracorporeal dialysis catheters or peritoneal dialysis catheters. Extracorporeal dialysis catheters are used for hemodialysis -ultrafiltration, hemodiafiltration, and continuous renal replacement therapy (CRRT) whereas peritoneal dialysis catheters are used for peritoneal dialysis: dialysis occurs across the peritoneal membrane.
Extracorporeal dialysis catheters– These catheters can be either non- tunneled or tunneled in nature.
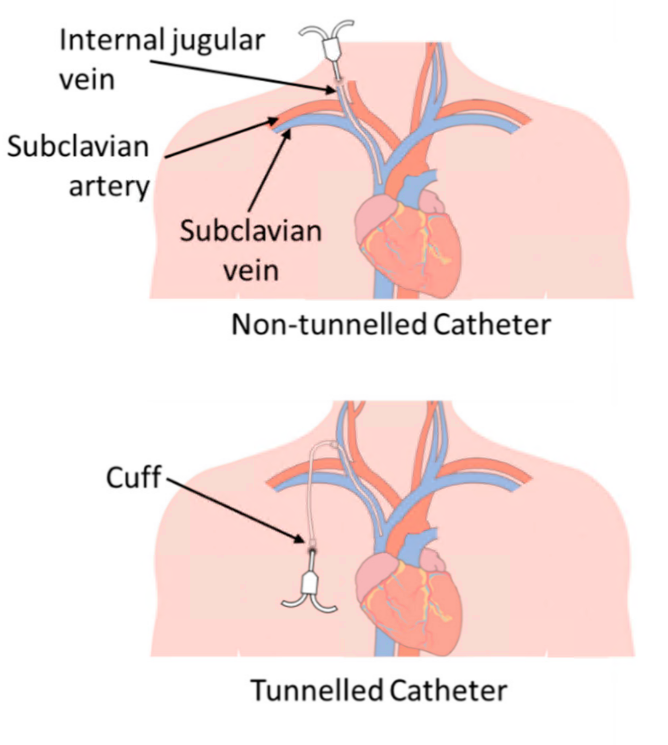
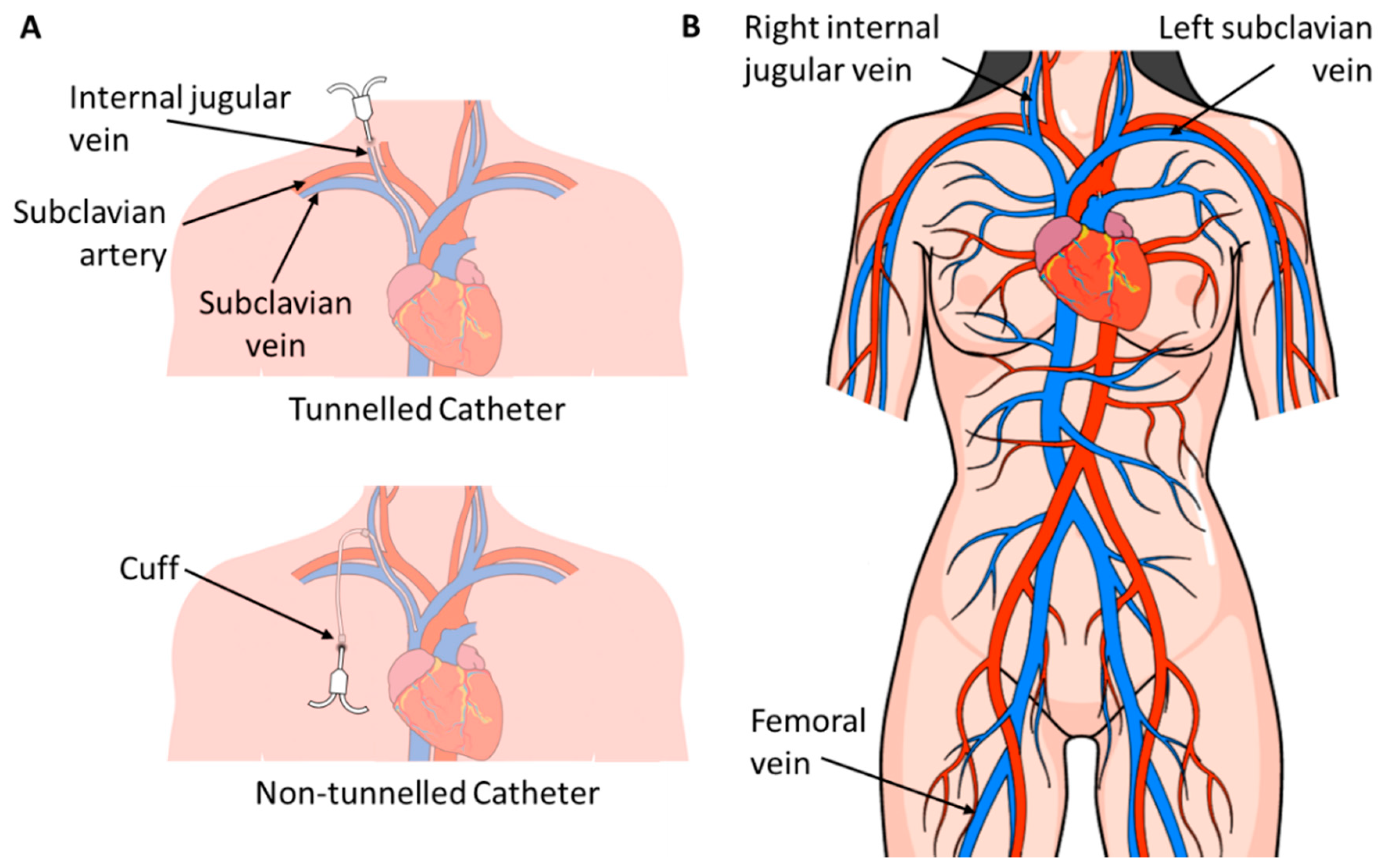
- Non-tunneled dialysis catheters are used for temporary or emergent situations (typically less than a week but can be used for up to less than 3 weeks according to some studies. However, sometimes with proper care they can be placed in for longer durations). These catheters are preferentially placed in the right internal jugular (IJ) vein> femoral vein> left IJ vein> subclavian vein (especially if placed on the dominant side). Figure 1 displays a schematic diagram of placement sites of dialysis catheters.
Complications of nontunneled catheters can be divided into acute and long term complications. Some acute complications include:
- Vascular injury (<1%)
- Hematoma (2% in the IJ and 5% in the femoral catheters)
- Pneumothorax
- Air embolism (<1%)
- Cardiac arrhythmias (can occur about 17-40%)
- Infections
Some long term complications include:
- Central venous stenosis
- Infections
The goal is to transition from nontunneled catheters, which are typically used in emergent cases, to more permanent accesses for chronic use such as tunneled hemodialysis catheters whenever possible.
- Tunneled Hemodialysis Catheters are used for long term (>2-3 weeks) or while waiting for arteriovenous (AV) fistulas to mature. Sites of placement in preferential order are:right IJ vein>left IJ vein> femoral vein. Ideally, the subclavian vein should be avoided given the risk for stenoses.
Indications for tunneled catheters include:
- Patient preference
- Scenarios in which dialysis is needed for than 3 weeks and an AV fistula is maturing
Complications of tunneled catheters include:
- Self limited oozing of blood at the exit site
- Prolonged oozing of blood
- Infections
Table 1 summarizes the differences between tunneled and non-tunneled catheter characteristics:
| Tunneled | Non-Tunneled | |
| Examples | Hickman’s®, Broviac®, Neostar, Leonard, and Groshong,Perm-Cath®, Hemosplit®, or Equistream® | Mahurkar, Vascath, Shiley |
| Lumen | Typically Double Lumen | Double or Triple Lumens |
| Size | 15.5 or 16 French | 8-13.5 French |
| Length | 12.5 cm-25 cm | 9-30 cm |
| Flow | >300 ml/min | 300-400 ml/min |
| Other Notes | The lumen is usually blunt, soft, and more flexible than nontunneled catheters | The design of the lumen can be straight or precurved and precurved lumens have been associated with decrease in removals |
- Peritoneal dialysis catheters that are used to access peritoneal space to instill dialysate fluid. The catheter can either be the rigid type (used in acute settings) or the more flexible and common type: Tenckhoff catheter. Figure 2 provides schematic representations of various types of PD catheters.

Some of the common indications for PD include:
- Patient preference (e.g. pediatric population some reasons include the less restrictive diet and a more normal lifestyle in comparison to hemodialysis)
- Bleeding diathesis or hemorrhagic conditions that prove it difficult for hemodialysis
- Cardiac conditions limiting hemodialysis (studies have shown that the continual removal with PD has shown benefits in refractory heart failure to aid in decreased hospitalizations and overall improved conditions)
Some complications of peritoneal dialysis include:
Some contraindications (relative) or considerations to take into account while thinking about peritoneal dialysis include:
- Severe malnutrition
- Proteinuria > 10 grams a day
- Advanced COPD
- Peritonitis
- Peritoneal fibrosis
- Adhesions
- Inflammatory Bowel Disease (IBD)
Table 2. displays different characteristics of peritoneal dialysis catheters.
| Peritoneal Dialysis Catheters | ||
| Portion | Options | Tidbits |
| Intra-abdominal segment | Straight or Coiled | Not a significant difference between the two in regards to peritonitis, exit-site infection, catheter failure or death |
| Subcutaneous Configuration | Straight vs Swan-Neck | No significant differences were noted; overall Swan Neck PD catheters were associated with better technique survival |
| Number of cuff | Single or Double | No significant differences in regards to outcomes were seen |
| Tip | Weighted vs Non-weighted | Weighted means 12 gm of Tungsten |
| Weighted allows for lower rates: migration, flow problems, transfer to HD, peritonitis, exit site infection, leaks | ||
| Material | Silicone vs Polyurethane |
Now, trainees can navigate the realm of dialysis catheters with more confidence.
Edited by Matthew A. Sparks, Amy Yau, Sudha Mannemuddhu, Anju Yadav, Swasti Chaturvedi, Gerren Hobby

{kind=link}
Article describes basic concepts but not sufficient information for patient management decisions.
In 2021, non-tunneled hemodialysis catheters should ONLY be used in hospitalized patients. If discharging patient, convert to tunneled hemodialysis catheter. And maintain vigilance on all catheters and removed as soon as fistula or PTFE graft is functional.
Very nice explanation
Very nice presentation